-
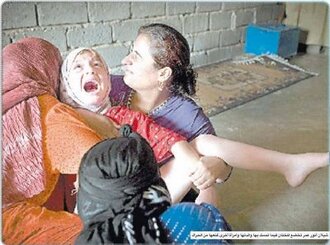 Stop Female Genital MutilationWhen a girl undergoes female genital cutting, some or all of her external genitals are cut away. This can be part or all of her labia, part or all of her clitoris and part or all of her clitoral hood (the prepuce). In its most extreme form, all of her external genitals will be cut away. This often happens in very basic circumstances with rudimentary tools; it is unlikely that there will be any anaesthetic or sterile conditions and often severe and life threatening complications follow FGM. In the harshest form of FGM, the wound that is left may be sewn closed with thorns or string and only a small hole is left for menstrual blood and urine. The wound then heals over and the scar tissue “seals” her vagina. When she is married she will then have to be cut open to make sexual intercourse possible, often on her wedding night. When she goes into labour, she has to be cut open again. After this she may be re-sewn and cut open again every time she conceives and gives birth. The World Health Organization (WHO) classifies FGM into four categories dependent on severity (initially there were three categories, the fourth was added later): Type I: Also known as clitoridectomy, this type consists of partial or total removal of the clitoris and/or its prepuce. Type II: Also known as excision, the clitoris and labia minora are partially or totally removed, with or without excision of the labia majora. Type III: The most severe form, it is also known as infibulation or pharaonic type. The procedure consists of narrowing the vaginal orifice with creation of a covering seal by cutting and appositioning the labia minora and/or labia majora, with or without removal of the clitoris. The appositioning of the wound edges consists of stitching or holding the cut areas together for a certain period of time (for example, girls’ legs are bound together), to create the covering seal. A small opening is left for urine and menstrual blood to escape. An infibulation must be opened either through penetrative sexual intercourse or surgery. Type IV: This type consists of all other procedures to the genitalia of women for non-medical purposes, such as pricking, piercing, incising, scraping and cauterization. The usual age for girls to be cut is between five and eight although in some communities, girls undergo FGM in their early teenage years and the procedure acts as a rite of passage into womanhood. Throughout history barbaric practices have been stopped mainly through a sustained process of education and legislation. FGM has continued because it has been a secretive and taboo subject. It is time to break the silence, educate and legislate, and eradicate FGM totally.40,203 of 45,000 SignaturesCreated by Beccy Roberts
Stop Female Genital MutilationWhen a girl undergoes female genital cutting, some or all of her external genitals are cut away. This can be part or all of her labia, part or all of her clitoris and part or all of her clitoral hood (the prepuce). In its most extreme form, all of her external genitals will be cut away. This often happens in very basic circumstances with rudimentary tools; it is unlikely that there will be any anaesthetic or sterile conditions and often severe and life threatening complications follow FGM. In the harshest form of FGM, the wound that is left may be sewn closed with thorns or string and only a small hole is left for menstrual blood and urine. The wound then heals over and the scar tissue “seals” her vagina. When she is married she will then have to be cut open to make sexual intercourse possible, often on her wedding night. When she goes into labour, she has to be cut open again. After this she may be re-sewn and cut open again every time she conceives and gives birth. The World Health Organization (WHO) classifies FGM into four categories dependent on severity (initially there were three categories, the fourth was added later): Type I: Also known as clitoridectomy, this type consists of partial or total removal of the clitoris and/or its prepuce. Type II: Also known as excision, the clitoris and labia minora are partially or totally removed, with or without excision of the labia majora. Type III: The most severe form, it is also known as infibulation or pharaonic type. The procedure consists of narrowing the vaginal orifice with creation of a covering seal by cutting and appositioning the labia minora and/or labia majora, with or without removal of the clitoris. The appositioning of the wound edges consists of stitching or holding the cut areas together for a certain period of time (for example, girls’ legs are bound together), to create the covering seal. A small opening is left for urine and menstrual blood to escape. An infibulation must be opened either through penetrative sexual intercourse or surgery. Type IV: This type consists of all other procedures to the genitalia of women for non-medical purposes, such as pricking, piercing, incising, scraping and cauterization. The usual age for girls to be cut is between five and eight although in some communities, girls undergo FGM in their early teenage years and the procedure acts as a rite of passage into womanhood. Throughout history barbaric practices have been stopped mainly through a sustained process of education and legislation. FGM has continued because it has been a secretive and taboo subject. It is time to break the silence, educate and legislate, and eradicate FGM totally.40,203 of 45,000 SignaturesCreated by Beccy Roberts -
 Save our Blood Plasma ServiceThe government is planning to sell off Plasma Resources UK, the firm responsible for supplying blood plasma products to the NHS, to a private contractor. We, the undersigned feel that this is unacceptable for the following reasons: 1. Blood plasma is essential for the treatment of many conditions, including burns, shock and major trauma; immune disorders and neurological conditions; protecting unborn children from haemolytic diseases. Possibly best known plasma product is Factor VIII used to treat around 3,000 haemophilia patients. 2. The profit impetus may compel any company taking over services to cut corners in order to make return. This could have devastating consequences for patient safety should contaminated, poorly packaged or improperly labelled products reach frontline healthcare services. The next part of this section is a fuller statement about Blood Plasma and why it is so important to stop the sell off of Plasma Resources UK. It shows how the Government has already split plasma services away from the National Blood Service so that part of what was a unified Blood Transfusion Service can be sold off for profit. Read on: First of all an apology. I started this petition on 38 Degrees after seeing and signing a similar one on the Government ePetition website. After doing a little research of my own and receiving an email via this site, it is clear that the Blood Transfusion Service (NHSBT) is not being sold off. However, Mr. Lansley has been party to breaking up NHSBT in 2011. It is the part that he has separated off that he is looking to sell off. That company is Plasma Resources UK (PRUK), the principal supplier of plasma and plasma products to the NHS. Blood and Plasma are obviously ‘joined at the hip’. When a donor gives a pint of blood, 55% of that fluid by volume is plasma. Much of today’s service is about producing blood and plasma products for the treatment of a wide range of patients. Treatments using plasma products are no less important than those using blood products. You have only to ‘google’ medical uses of plasma to find out the wonderful way its products can influence patients lives, such as the treatment folk suffering from burns, shock and major trauma; immune disorders and neurological conditions; protecting unborn children from haemolytic diseases. Possibly best known plasma product is Factor VIII used to treat around 3,000 haemophilia patients. The work of producing these valuable plasma products (there are hundreds of them) has been carried out by the Bio Products Laboratory (merged with the Blood Service in 1993 and now called Bio Products Limited (BPL)). Plasma Resources UK (PRUK) is the Health Dept company that manages the supply of blood plasma from the US through US based British owned company DCI Inc, which has been necessary since the BSE outbreak and concerns about people developing vCJD. For some years there has been a particular strategy to reduce the dependency of NHSBT's blood products division (BPL) on government subsidies. ‘Our Fractionated Products division (BPL) operates in competitive markets across the UK and globally with other multi-national pharmaceutical companies. A key strategic goal has been to move this part of our organisation into a profitable trading position. This was achieved during 2008/09 thanks to the continued growth in sales and throughput. Our future plans seek to sustain and build on this performance.’ Just a year later this part of the Blood Service was hived off to a separate division from NHSBT: ‘On 1 January 2011 Bio Products Laboratory was transferred into a new legal entity, Bio Products Laboratory Limited, a 100% owned subsidiary of Plasma Resources UK Limited (PRUK), which is 100% owned and managed by the Department of Health.' There are concerns about ‘blood and plasma markets’ in the US. The cost to DCI includes payment to donors. The market has also been described as working like a monopoly or cartel, where at one extreme price can be fixed or competition can be fierce leading to among other things attempts to reduce costs and all the inherent dangers in that. This market in the USA has been described as representing “everything wrong with American-style capitalism”. It is too early to know what relationship a privatised PRUK would have with the NHS and hence what the implications to the NHS might be in terms of cost and guarantees about supply. I recall that a few years ago there were fears of a flu epidemic (I think) and it was found that vaccine originally destined for this country was redirected to other countries where the Pharmaceutical Company could get a higher price. Could the same happen with a privatised Plasma Products company? If the time comes when we can recommence plasma donations in this country, would anyone sign up if their altruistic gift was given to a company concerned with making a profit from it?5,860 of 6,000 SignaturesCreated by Geoff Dunbar
Save our Blood Plasma ServiceThe government is planning to sell off Plasma Resources UK, the firm responsible for supplying blood plasma products to the NHS, to a private contractor. We, the undersigned feel that this is unacceptable for the following reasons: 1. Blood plasma is essential for the treatment of many conditions, including burns, shock and major trauma; immune disorders and neurological conditions; protecting unborn children from haemolytic diseases. Possibly best known plasma product is Factor VIII used to treat around 3,000 haemophilia patients. 2. The profit impetus may compel any company taking over services to cut corners in order to make return. This could have devastating consequences for patient safety should contaminated, poorly packaged or improperly labelled products reach frontline healthcare services. The next part of this section is a fuller statement about Blood Plasma and why it is so important to stop the sell off of Plasma Resources UK. It shows how the Government has already split plasma services away from the National Blood Service so that part of what was a unified Blood Transfusion Service can be sold off for profit. Read on: First of all an apology. I started this petition on 38 Degrees after seeing and signing a similar one on the Government ePetition website. After doing a little research of my own and receiving an email via this site, it is clear that the Blood Transfusion Service (NHSBT) is not being sold off. However, Mr. Lansley has been party to breaking up NHSBT in 2011. It is the part that he has separated off that he is looking to sell off. That company is Plasma Resources UK (PRUK), the principal supplier of plasma and plasma products to the NHS. Blood and Plasma are obviously ‘joined at the hip’. When a donor gives a pint of blood, 55% of that fluid by volume is plasma. Much of today’s service is about producing blood and plasma products for the treatment of a wide range of patients. Treatments using plasma products are no less important than those using blood products. You have only to ‘google’ medical uses of plasma to find out the wonderful way its products can influence patients lives, such as the treatment folk suffering from burns, shock and major trauma; immune disorders and neurological conditions; protecting unborn children from haemolytic diseases. Possibly best known plasma product is Factor VIII used to treat around 3,000 haemophilia patients. The work of producing these valuable plasma products (there are hundreds of them) has been carried out by the Bio Products Laboratory (merged with the Blood Service in 1993 and now called Bio Products Limited (BPL)). Plasma Resources UK (PRUK) is the Health Dept company that manages the supply of blood plasma from the US through US based British owned company DCI Inc, which has been necessary since the BSE outbreak and concerns about people developing vCJD. For some years there has been a particular strategy to reduce the dependency of NHSBT's blood products division (BPL) on government subsidies. ‘Our Fractionated Products division (BPL) operates in competitive markets across the UK and globally with other multi-national pharmaceutical companies. A key strategic goal has been to move this part of our organisation into a profitable trading position. This was achieved during 2008/09 thanks to the continued growth in sales and throughput. Our future plans seek to sustain and build on this performance.’ Just a year later this part of the Blood Service was hived off to a separate division from NHSBT: ‘On 1 January 2011 Bio Products Laboratory was transferred into a new legal entity, Bio Products Laboratory Limited, a 100% owned subsidiary of Plasma Resources UK Limited (PRUK), which is 100% owned and managed by the Department of Health.' There are concerns about ‘blood and plasma markets’ in the US. The cost to DCI includes payment to donors. The market has also been described as working like a monopoly or cartel, where at one extreme price can be fixed or competition can be fierce leading to among other things attempts to reduce costs and all the inherent dangers in that. This market in the USA has been described as representing “everything wrong with American-style capitalism”. It is too early to know what relationship a privatised PRUK would have with the NHS and hence what the implications to the NHS might be in terms of cost and guarantees about supply. I recall that a few years ago there were fears of a flu epidemic (I think) and it was found that vaccine originally destined for this country was redirected to other countries where the Pharmaceutical Company could get a higher price. Could the same happen with a privatised Plasma Products company? If the time comes when we can recommence plasma donations in this country, would anyone sign up if their altruistic gift was given to a company concerned with making a profit from it?5,860 of 6,000 SignaturesCreated by Geoff Dunbar -
Compulsory personal therapy for trainee and qualified practicing counsellorsCurrent research shows that in U.K., more than 62% of clinical psychologist report having experienced mental health difficulties at some point in their career. With the implementation of the SCoPED frame of work the counselling and psychotherapy industry in the U.K. is one step closer to being regulated and receiving the deserved attention. In a society where mental health is beginning to be appreciated in all sectors and aspects of one's life, it is irresponsible that regulator organisations, which are part of the SCoPED frame of work, such as the BACP, ACC, HGI & NCS, facilitate trainees and "registered/accredited members" who are not undergoing personal therapy as an integrated part of their training and professional development; to practice in paid client work obtained through directories managed by the said organisations. Such can be verified by reading the SCoPED PowerPoint (slide 14) frame of work published ON THE WEBSITES of those organisations mentioned. When it comes to ethical and safe therapy offered to vulnerable people, there should be no buts or ifs. Clients of any kind have next to no understanding of what constitutes a professional counsellor, nor should they be held responsible for doing so. Counsellors and organisations who profit from the service they provide are entirely responsible and, above all should be making sure of doing no harm. Many courses accredited by those organisations mentioned do not integrate personal therapy in their training, placing students and potential clients at great risk. People should join my campaign to support a safer and more regulated industry. Supervisors would know the risks involved and should back me up to protect their supervise. Institutions benefitting from the high cost of the training they offer are obliged to provide an ethical frame of reference to their students before they reach the public. Regulators like the UKCP and BPS, who fortunately require personal therapy, should help to set the standards that they themselves believe in and sign up for the petition.83 of 100 SignaturesCreated by Gianluca Giordano
-
Don't let Palantir near our NHSPalantir was formed by the CIA and its expertise is in surveillance and border security, NOT health or patient data. Palantir is fully American owned. There is no guarantee that your patient data won't be harvested and stored outside the UK. This would make it very difficult to police the security of your data. Although the data is meant to be anonymised various organisations could get hold of the means of restoring personal data from the database.24 of 100 SignaturesCreated by Bruce Morton
-
All Nurses to receive mandatory moving and handling training, and refresher coursesI have two sons who both live with Duchenne Muscular Dystrophy. We are grateful for the NHS and have always received fantastic care any time we have needed it. There is just one problem, most of the Nurses we have encountered in both Paediatric and Adult Departments have little experience in Moving and Handling patients who require hoisting. This is due to a comparatively small number of patients requiring this, however for those patients who do, this is essential. Nurses really ought to receive moving and handling training, including with slings and hoists, and should have access to refresher courses at least once a year, to ensure that every patient receives the best care possible. Every patient deserves the best care, and when Nursing Staff have little or no experience this can result in injury to the patient and themselves.1 of 100 SignaturesCreated by Muggins de Jinx
-
Social Prescription Must Be Added to the UK's Health Service.The NHS was founded as a two pronged system. There was the NHS - The national Health Service, and there was the NHS - The Natural Health Service. The second NHS is far less well known but equally important. The idea behind the movement was to give all people access to the natural landscape around us for the benefits it gives to us mentally and physically. This was important as people has just returned from second world war - people had died for this land and they deserve access to it. The move to give people access to our natural landscape was blocked by the House Of Lords (as you can imagine they don't want people snooping around there land). The point here is that the NHS was founded under the principle that we would have access to landscape and people. Today, social and nature prescription is on the rise but still has little to no space in the public sphere as a genuine way for us to tackle our health crisis. We need it as a part of our preventative and ongoing care for people with issues from mental health to physical ailments. It's cheaper than medecine and strengthens community bonds and resilience.24 of 100 SignaturesCreated by Ed Smit
-
Please don't move the goalpostsTargets, (whether or not they are achieved by the NHS), help us to judge the performance of the NHS over time.4 of 100 SignaturesCreated by Santanu Pal

-
Support GP practices - Partners not private enterpriseA family doctor, who knows your medical history, is vital to our health and well being and should be available for all of us. Our GP practices are under more pressure than ever before. There is a national shortage of GPs and central government is undermining and failing to support surgeries which are led by GP partners - instead they are encouraging the privatisation of GP surgeries leading to disastrous consequences for patient care. Companies such as Virgin, Boots and US company Operose are buying up GP practices when the GPs eventually give up due to underfunding. The private Companies may even get more funding than the GPs were given in some cases. Patients then find that they are unable to get appointments and the same level of care they received before. One practice in Kent, bought up in 2016, went from outstanding, when run by GPs, to inadequate in the 18 months after it was bought up by a private firm. Other GP surgeries have been highlighted on Panorama, showing how the private companies make more money by employing fewer GPs ( perhaps as little as 1 per practice) and making up the needs with less highly trained and much less well paid physician associates who need support, which they may or may not get, from a GP so they don't make mistakes with diagnosis or patient care. The government is encouraging a two tier system to develop. In the near future, if this trend is not reversed, only rich people with access to private health care will be able to get reliable health care when they need it. My own GPs have criticised the political decisions being made which are making it so difficult for the doctors - they say this started in the Thatcher years but every government since has contributed to the problem. One of them described it as "heartbreaking" because the poor will not be able to get adequate care and many may die unnecessarily. The service is at breaking point already. Almost all the appointments at my surgery are now telephone only and this can lead to mistakes being made. I would like to see these decisions reversed by the government and I call on the Health Secretary to take urgent action. It is completely inappropriate for private companies to be running GP surgeries for big profit while neglecting patient care. Central government should be adequately supporting GP led and run partnerships- they are the ones who know how to do the job properly and they are invested in the work. Big business just doesn't care. It's profits before people. If we all petition the Government on this issue, they have to take notice as privatisation of the NHS through the back door is an election loser. I want this to be debated in the House of Commons. This is a national issue which affects all of us.9 of 100 SignaturesCreated by Moira Oram
-
NHS Coil Removal Waiting Times Are As Long As A YearSince the summer I have been making contact with my local GP to book an appointment to have my current coil (expiring in November) replaced. I was made aware by female family/friends that I should make contact with my GP as far in advance as possible as the waiting list for the coil is extremely long. After calling my GP in the summer I was told that I had made contact too early and I should call again one/two months in advance to book in. I followed these instructions and was eventually added to the coil waiting list in September. After chasing up my case in October and then again in early November I was informed by the administrator in charge of the 'Coil waiting list' on both occasions that she could still not offer me an appointment as there are still no slots available. I raised my concern about the fact my coil is now expiring in a matter of weeks and as a result I wouldn't be protected from getting pregnant unless my husband and I use condoms. The clinician advised that there is nothing she could do about getting me an appointment any earlier as the waiting list is very long and there are only two practitioners who take appointments for the coil. I asked if she could give me any sort of time frame as to how long I would have to continue with my expired coil and she couldn't give me an answer. In an attempt to be proactive, I made contact with my local Sexual Health Clinic to enquire if I could make an appointment with them to have my coil removed. They informed me that this is not a service they offer anymore and I needed to make an appointment with my GP. I have since researched the 'NHS coil waiting list' and found that it can be as long as 6 months to a year women have to wait to have their coil removed. More clinicians in GP practice need to become qualified to take appointments relating to the coil. The 'NHS coil waiting list' is an issue directly related to female empowerment. The current system within the NHS is completely ineffective and has personally left me feeling completely out of control of my own body. Choosing the correct method of contraception is an extremely important issue that every woman in the UK goes through at some point during their life. As a married woman in my late 20's, I am settled with a long term partner but not yet ready to start a family. The coil is the correct method of contraception for me at this stage of my life, however I am unable to access it. Furthermore I have a coil that will be expiring imminently and I am unable to book an appointment to have it removed in time, and there is absolutely no time scale that can be provided by my GP as to when I will get an appointment. Women in the UK should not have to wait for this ridiculous amount of time to gain access to contraception. Not only is the process of trying to get an appointment for the coil emotionally draining and exasperating, it is unbelievable that we are in 2022 and women in this country are left to feel completely out of control in matters to do with their own body.72 of 100 SignaturesCreated by Sarah Parker
-
New Sutton Hospital NowThis new hospital is urgently needed to bring our NHS facilities into the 21st century and to provide top quality care. In the meantime many people will continue to suffer and lives will continue to be unnecessarily lost. Staff morale is at an all time low because of this.5 of 100 SignaturesCreated by Tim Manley
-
Annual Bowel Cancer ScreeningI was diagnosed with Bowel cancer aged 37 after being misdiagnosed with diverticulitis. Misdiagnosis is common in people under 50 because they are considered too young to have Bowel cancer and red flags are ignored. There is no age limit to Bowel cancer. There are approximately 42,886 cases of Bowel Cancer each year. Bowel Cancer has a 54% survival rate, if caught early enough. There is no action you can take to prevent bowel cancer, it is considered “The smoking old man’s meat eating cancer” which is simply not the case for everybody. My doctors have not been able to identify a single reason why I have this cancer and I don’t fit the bill at all. It is possible it has been present for years even though I am “too young” to have it. My blood loss and pain was thought to be a gynaecological issue and I was diagnosed with a Anaemia. Even a perforated bowel didn’t seem to ring alarm bells. Cancer was not a consideration. We now know I was losing blood via stools, without realising and a tumour had perforated my bowel, eventually causing excruciating pain. Screening could have detected this and I may not have had to have part of my colon removed in emergency surgery and have to live with a stoma. I want it made possible to stop this cancer in its tracks before it gets to my stage or further for anybody else. After all, if Bowel cancer develops it can also spread to lymph nodes then onto other organs which can be even more devastating. Let’s try to prevent more Bowel cancer related deaths in the future by screening adults aged over 30 annually and allowing anyone over 18 to opt in as well. Feel free to follow my journey on Instagram @paloma_the_stoma2211 of 100 SignaturesCreated by Amy Prowse
-
Stop Ofgem from committing murderMany people on low incomes will lose their lives through hypothermia, as they will not be able to afford heating. Many more older people will just try and wrap up warm instead of putting the heating on because they can't afford the gas, or electric. Many disabled people on low incomes will have to choose between heating or food. This is corporate murder. The outcome of this is a massive rise in the death rate this winter. I myself am looking at a winter of severe pain with little to no heating each day. My mother is likely to just not turn the heating on and wrap up as warm as possible as she is of the wartime generation. I fear that she will not survive the next winter. Many of her generation, and their children on low incomes (state pensions) will likely do the same as they will not be able to afford heating this winter. Please do not start up a similar petition as it will weaken this petition. Instead share this one so as many people can sign it, and it gets brought before the house of commons.11 of 100 SignaturesCreated by Raven Pen-Orthyn
Hello! We use cookies to improve your experience by providing insights into how the site is being used. Find out more.